
On February 26, at an "Eat Real Food" rally at Brazos Hall here in Austin, Health Secretary Robert F. Kennedy Jr. told an fawning crowd that Dunkin' Donuts and Starbucks should be made to produce "safety data" proving their high-sugar beverages are safe for human beings to consume . A Dunkin' frozen drink, he noted, can contain 115 grams of sugar. Under his leadership of the Department of Health and Human Services, companies would face a rigorous review which, apparently, was being bypassed on the regular.
The internet found this very funny. On the other hand, the public health community let the whole thing slide, which I think is a total mistake. Kennedy is not simply wrong, but wrong in a very specific way that tells you something important about how health misinformation works in the hands of someone who knows just enough to sound credible.
Philosophers have a name for this this maneuver: the motte and bailey. Medieval castle complexes were built with a fortified stone tower, called the motte, which was surrounded by an open courtyard called the bailey. The bailey was where the everyday life happened, like the livestock and the market and the people going about their business. The motte was where you went when things got dangerous. Kennedy's rhetoric works the same way.
His motte is unassailable. The American food environment absolutely contributes to chronic disease burden. Ultra-processed food consumption in the United States ranks among the highest in the world. The GRAS self-determination process has legitimate problems that the Government Accountability Office and former FDA officials have both flagged on the record. None of that is wrong, and not one of Kennedy's inventions.
GRAS stands for “generally recognized as safe.” Under FDA rules, companies can designate certain ingredients as safe based on scientific consensus or long history of common use, without submitting those ingredients for formal FDA review. The process was designed for well-established substances like vinegar or black pepper. Critics, including the Government Accountability Office, have argued that manufacturers have used it to introduce novel additives into the food supply with minimal independent oversight.
Kennedy’s bailey is his claim that Dunkin’ is hiding safety dossiers that would prove that a beverage is dangerous. So, the absence of said dossier for table sugar should be considered regulatory negligence and demanding such a thing is the most reasonable thing a public health authority can do. When pressed, Kennedy falls back on the claim that American food is making people sick and acts as though that was the argument all along. The bailey sounds just enough like the motte that the audience will never notice the switcheroo.
His demand has a structural flaw worth getting into, albeit carefully. Kennedy is applying a regulatory standard designed for food additives to an ingredient that is not, in any meaningful legal or scientific sense, a food additive. Sugar is a conventional ingredient with centuries of established use. The FDA does not require manufacturers to produce safety dossiers proving sucrose is safe at every possible dose, because the regulatory framework governing conventional ingredients was never built to generate that evidence. That dossier does not exist at any company, was never required, and could not be produced under the current system. The system Kennedy is invoking was never designed to work the way he implies.
The flaw is deeper than simple regulatory category confusion. Kennedy is applying the logic of drug safety to a question about food, and the two work differently. When a pharmaceutical company studies whether a drug is safe, they ask whether this compound causes harm at this dose, in this body, over such-and-such a period of time. Food does not work that way. The question researchers ask is whether people who eat certain ways over years and decades develop different health outcomes than people who do not. One bad meal is not a clinical event. A decade of bad meals might be.
HOW FOOD RESEARCH DIFFERS FROM DRUG RESEARCH: Drug safety trials can isolate a single compound, control the dose precisely, and measure outcomes over a defined period. Dietary research cannot do any of those things cleanly — people eat dozens of foods daily, in combinations that shift constantly, across lifetimes of exposure. This is why nutritional epidemiology studies populations and patterns rather than individual substances and doses. The two fields ask genuinely different questions, and importing the evidentiary standards of one into the other produces demands that sound rigorous but are structurally impossible to meet.
Consider a donut. A single high-sugar beverage is not a meaningful health risk for most people. Personally, I rarely drink sugary drinks, but occasionally I like to treat myself. Does that mean it’s going to kill me? When researchers find links—associations, really—between sugar-sweetened beverage consumption and metabolic disease, they are studying populations who drink them on a regular basis for years. The epidemiology of this measures dietary pattern, not single occasions like when someone treats themselves for getting an “A” on an exam. Someone who stops at Dunkin’ on a Saturday morning is not registering on any population-level risk curve. The person who does it every single morning before work for a decade is a different story, and the gap between those two people cannot be found anywhere in a safety dossier, because it is the wrong tool for the problem.
By reframing a dietary pattern problem as a chemical safety problem, Kennedy succeeds in something that looks like consumer protection but acts as misdirection. The anxiety his rhetoric creates has its own health costs. Framing a single snack as a form of toxic exposure, consumed by someone who knows nothing of the safety data, is a bad way to think about eating.
Orthorexia is an eating disorder characterized by an obsessive focus on food purity and safety. Unlike anorexia, which is driven by fear of weight gain, orthorexia is driven by fear of consuming anything perceived as harmful or impure. Sufferers may restrict their diets to the point of malnutrition while believing they are being healthy. Public rhetoric that frames ordinary food consumption as a potential toxic exposure can reinforce the cognitive distortions that drive orthorexic behavior.
More consequentially, this pushes the public’s attention towards a question with no good answer, such as where is Dunkin’s safety dossier, and away from questions we do have answers for, like why is high-frequency consumption of these products the path of least resistance for a large portion of the population, and how much of that are deliberate decisions about pricing, availability, and product engineering rather than individual choice?
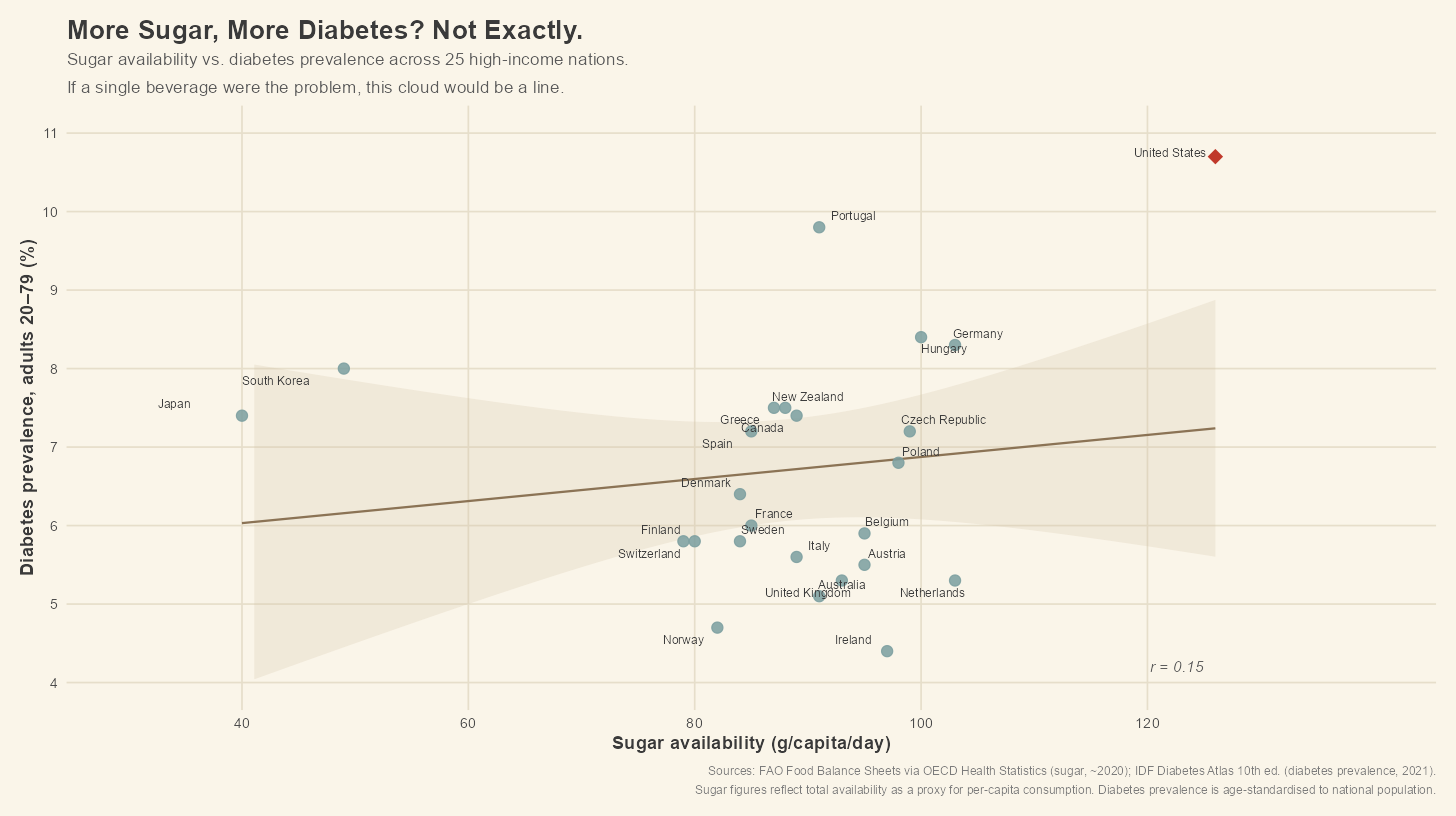
Plotting sugar availability per capita against type 2 diabetes prevalence across 25 high-income nations, using FAO food supply figures and IDF Diabetes Atlas estimates, gives us a correlation of 0.15. Sugar availability explains roughly 2% of the variation in diabetes prevalence among these countries. The United States sits where you would expect, high sugar and high diabetes, and if you look at it quickly, it seems to support Kennedy’s case. Germany and the Netherlands consume sugar at nearly the same levels as Americans, yet they land almost smack dab below the United States on diabetes. Portugal consumes less sugar than the United States and nearly matches its diabetes rate. Japan and South Korea consume far less sugar than any Western European country and still exceed seven percent prevalence, higher than several nations eating considerably more. What you get when you plot this is a cloud, not a line, but the cloud is the point.
A NOTE ON WHAT r = 0.15 MEANS: A Pearson correlation coefficient measures how closely two variables move together, on a scale from -1 to 1. A value of 1 means they move in perfect lockstep. A value of 0 means they have no relationship at all. A value of 0.15 — which is what we find between sugar availability and diabetes prevalence across these 25 countries — is close enough to zero that it describes an essentially random scatter. Squaring that number gives you the proportion of variation in one variable explained by the other: 0.15 squared is roughly 0.02, meaning sugar availability accounts for about two percent of the differences in diabetes prevalence across these nations. The other 98 percent is doing the work.
[Chart: Sugar availability vs. diabetes prevalence across 25 high-income nations]
This not to say that sugar doesn’t matter to metabolic health. Sugar intake at population scale, sustained over time, contributes to chronic disease burden, and the science supporting that is in no way in dispute here. What the chart shows is that sugar availability, taken alone as a country-level variable, predicts almost nothing about how diabetic the populace gets, which means the causal story is much tougher than any one ingredient, and interventions built on Kennedy’s model would be shooting at the wrong target.
The concern here is not toxicological, but structural. Regulations are better spent elsewhere. So the better question is why, for a substantial portion of the American population, the high-sugar option is the cheapest, the most available, and those designed to make the consumer unable to “just have one.” That gets into the topic of food deserts and pricing, through the neurochemistry of hyperpalatable food design and advertising aimed at kids, and through decades of underinvestment in neighborhoods where physical activity is available. Regulatory pressure applied to any of those would move the dial on this problem.
Kennedy is not wrong that the food supply deserves a serious look at. The GRAS process has problems, but they involve novel emulsifiers, preservatives, and flavoring agents, not in the cup of sugar you borrow from your neighbor. Using a valid critique of GRAS with an example that has nothing to do with it is a rhetorical move, not a policy one, and it takes the credibility from a real debate to prop up a claim that cannot stand on its own.
The most damaging part of Kennedy's rhetoric on the matter is not that it is false. Falsehoods are correctable, afterall. The damage is that people who believe him and try to act on it will spend all their energy solving the wrong problem. A safety dossier on sugar tells you nothing about why millions of people eat poorly every day. This is the problem worth solving. Demanding one is just performative. The conversation that might move the needle starts the moment people stop watching the performance and look past it.
Sources: FAO Food Balance Sheets via OECD Health Statistics (sugar availability, ~2020); IDF Diabetes Atlas 10th edition (diabetes prevalence, 2021); Sun H et al., Diabetes Res Clin Pract. 2022;183:109119.