
The only documented case of a creature with strong opinions about whose blood it would accept is none other than Dracula, and even he was never very picky. Sure, he had standards, but he did not, across two centuries of fiction and roughly nine hundred film adaptations, ever hesitate at the jugular to ask whether the victim had received a COVID-19 vaccine.
Oklahoma state Representative Justin Humphrey had stronger feelings about this than the Count. In January 2026, he introduced House Bill 3196, which proposed that the Oklahoma State Department of Health create a blood bank stocked solely with donations from people who had not received a COVID-19 vaccine.¹ He told reporters he did not want vaccinated blood in his body, and that if he were ever in a wreck, he wanted to know in advance where he would get his blood. When physicians explained that no available test can distinguish the antibodies of a vaccinated person from those of someone who contracted COVID-19 in the wild, Dr. Steven Crawford of the University of Oklahoma told Oklahoma Voice the bill "would essentially shut down all blood banks because there's no way they could comply."¹ A day after the story broke, Humphrey faced enough public finger-wagging that he backed down from the legislation and said he was just trying to start a conversation.
As it turns out, the conversation he started was with hematologists across the state, who had to stop seeing patients to explain antibodies to a legislative committee.
The COVID-19 mRNA vaccines are injected into muscle. The mRNA enters muscle cells at the injection site, instructs those cells to produce spike proteins, which prompts an immune response, and then it breaks down. The mRNA does not replicate, cannot integrate into DNA, and does not transfer through a blood transfusion.² The immune response the vaccine generates does produce antibodies, which do circulate, but even those do not survive the preparation process blood goes through before it reaches a patient. A prospective study measuring anti-SARS-CoV-2 IgG levels found antibodies present in 93.5% of donor serum samples and absent in all processed red blood cell units; the filtration and plasma depletion steps removed them in every unit tested, and red blood cells carry no antibodies regardless of donor vaccination status.²
A retrospective study published in Transfusion tracked outcomes in 7,773 hospitalized patients who received plasma or platelet transfusions from vaccinated donors between June 2020 and March 2022, measuring rates of blood clots, respiratory complications, and death. The researchers found no association between receiving blood from vaccinated or previously infected donors and any of those outcomes.³
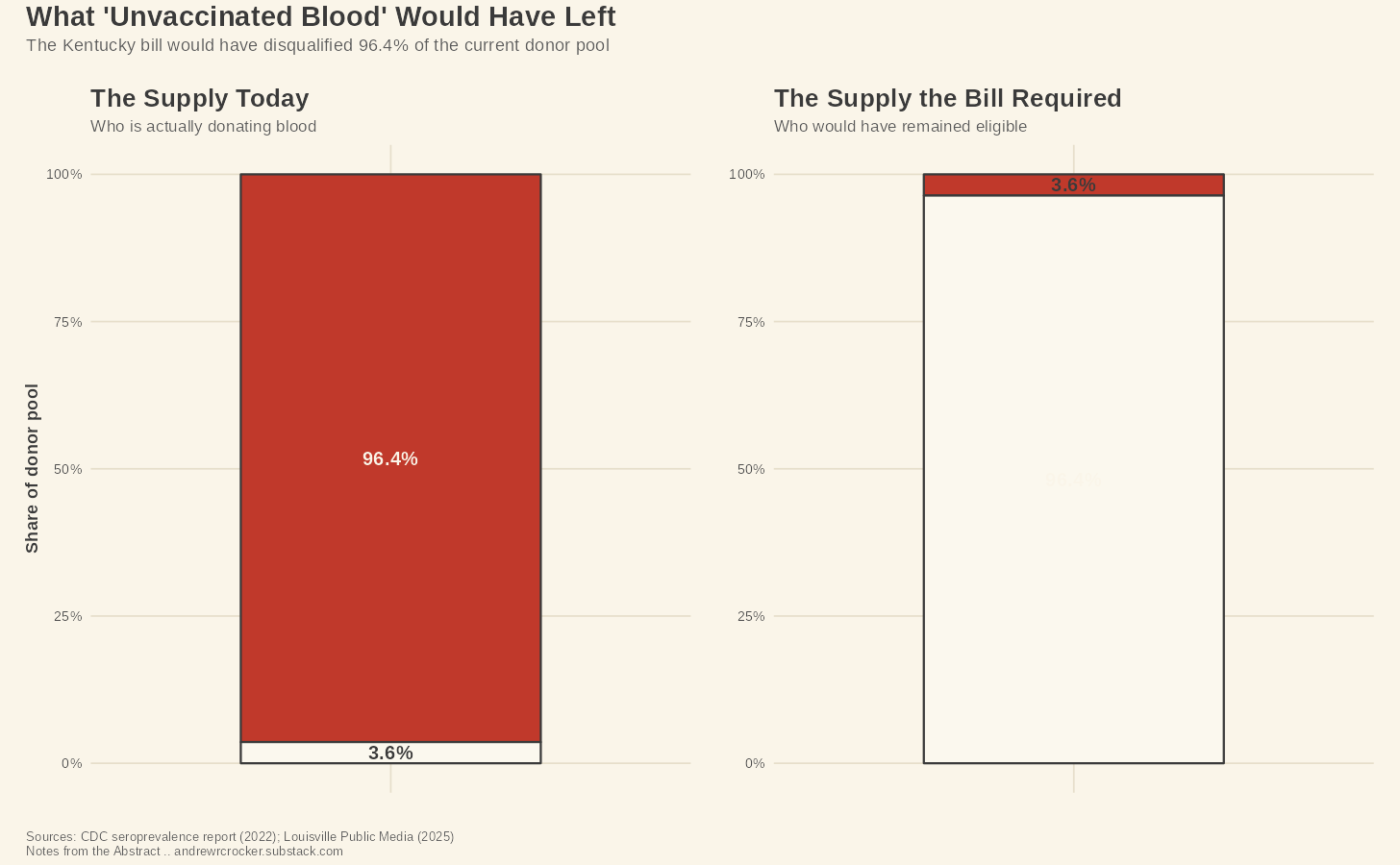
If you apply the word "unvaccinated" to blood, it doesn’t mean anything. A 2023 CDC MMWR report found that approximately 96.4% of blood donors carry COVID-19 antibodies, through vaccination, prior infection, or both.⁴ The pool of donors who could qualify as "unvaccinated" under any working definition of the term is 3.6% of the current supply.
The U.S. collects roughly 13.6 million units of whole blood and red blood cells annually from approximately 6.8 million donors.⁵ Against a system that transfused 10.3 million units in 2023 alone,⁶ 3.6% of the supply is 489,600 units. That does not even begin to meet the requests being made, let alone the volume that would exist if six states had successfully mandated compliance. The system has no reserve to draw on. The average donor age climbed from 44 in 2013 to 51 in 2023, the rate of first-time donors who never return rose from 35% to 55% over that same decade, and only about 3% of age-eligible Americans donate in a given year.⁶
Humphrey filed his little bill into a system already running at a 3.6% margin of error.
Lawmakers in Connecticut, Kentucky, Montana, Oklahoma, Tennessee, and Wyoming introduced bills requiring hospitals to honor requests for blood from unvaccinated donors. Thankfully, none of them passed. The Kentucky bill was the most specific; it would have blocked transfusion of blood testing positive for COVID-19 antibodies or synthetic mRNA, pending development of a test capable of detecting mRNA in donated blood.⁷ Obviously, no such test exists. So, the bill's sponsor later said the mRNA restriction had been a mistake.
The bill would have required compliance with biology you cannot measure in order to protect against a risk the evidence doesn't support.
Patients were already paying for that misinformation in operating rooms. Vanderbilt University Medical Center recorded 48 directed donation requests from 15 recipients over 2024 and 2025, with requests climbing from 4 in 2024 to 11 in 2025.⁸ All 48 were because the patients were concerned about receiving vaccinated blood. Thirteen patients received blood donated specifically by family members they knew to be unvaccinated. Two of the 15 recipients suffered serious complications; one developed anemia, the other went into hemodynamic shock.
Extensive studies cited in the Vanderbilt review found that first-time parental donors, the category most directed donation requests produce, carry markers for transfusion-transmissible infections at a rate of 8.6%, compared with community donors.⁸ The blood being sought as safer is statistically more likely to carry a pathogen that the standard screening process was built to catch.
Jeremy W. Jacobs, an assistant professor of pathology, microbiology, and immunology at Vanderbilt, wrote in STAT News that managing these requests pulls transfusion medicine specialists away from patients who need them and forces institutions to build counseling protocols for a concern the 2025 Transfusion study resolved before the first bill was filed.⁹ No public legislative fiscal note on the six bills addressed the staff time these requests consumed.
People who refuse vaccinated blood are not making a rational choice. The belief in "unvaccinated blood" is factually wrong. The Vanderbilt data recorded what happened when two patients almost died waiting for blood their bodies could not distinguish from what they refused.
What’s more, the clinical record has nowhere to put any of that. When a patient refuses a standard transfusion, waits for a donor to be screened, and then goes into hemodynamic shock during surgery, that encounter generates codes. Coders assign a code to the shock. The operative note may document the surgical delay, and their refusal might come up in a clinical note if the transfusion medicine specialist wrote up the counseling conversation in enough detail for a coder to act on it. Whether any of that documentation produces a structured code depends on whether the facility's coding staff had reason to look for it and a code to assign.
ICD-10-CM, the coding system that turns clinical encounters into structured data, has no code that captures a procedure delayed because of a patient-requested directed donation on vaccine-refusal grounds. The complication that ends up in the principal diagnosis carries no trace of what produced the delay. A researcher pulling discharge data five years from now will find hemodynamic shock and a surgical case.
The belief system that caused the delay has no classification in the record and no advocate pushing for one. Patients who went into shock waiting for unvaccinated blood will have their outcomes attributed to the surgery, not to the refusal that delayed it.
The pattern will not pop up in any surveillance system that reads coded data, because the coded data will not contain it. Clinicians watching a patient deteriorate are not building a longitudinal record of how misinformation moved through that patient's decision-making—they’re just trying to stop the bleeding.
Lawmakers ignored biology and tried to mandate a preference based on misinformation. The patients in the Vanderbilt study, who went into shock, waited for blood that was, in the only clinically relevant sense, identical to what they refused, waited because the word "unvaccinated" felt like a guarantee.
The guarantee was not in the blood.
References
¹ Murphy E. Oklahoma lawmaker proposes blood bank for vaccine-free blood. Oklahoma Voice. January 21, 2026. https://oklahomavoice.com/briefs/oklahoma-lawmaker-proposes-blood-bank-for-vaccine-free-blood/
² Zdanowicz A, et al. Absence of blood donors' anti-SARS-CoV-2 antibodies in pre-storage leukoreduced red blood cell units indicates no role of passive immunity for blood recipients. PMC. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10799091/
³ Roubinian NH, et al. Study confirms that COVID-19 vaccines, past infection pose no risk to transfusion recipient safety. Transfusion. 2025. https://www.aabb.org/news-resources/news/article/2025/03/04/study-confirms-that-covid-19-vaccines--past-infection-pose-no-risk-to-transfusion-recipient-safety
⁴ Tenforde MW, et al. Estimates of SARS-CoV-2 seroprevalence and incidence of primary SARS-CoV-2 infections among blood donors, by COVID-19 vaccination status — United States, April 2021–September 2022. MMWR Morb Mortal Wkly Rep. 2023;72(22):601–607. https://www.cdc.gov/mmwr/volumes/72/wr/mm7222a3.htm
⁵ American Red Cross. US blood supply facts. https://www.redcrossblood.org/donate-blood/how-to-donate/how-blood-donations-help/blood-needs-blood-supply.html
⁶ AABB. AABB24: what new data says about the state of the blood supply. October 21, 2024. https://www.aabb.org/news-resources/news/article/2024/10/21/aabb24--what-new-data-says-about-the-state-of-the-blood-supply
⁷ Louisville Public Media. Ky lawmaker behind bill limiting blood donations from COVID-vaccinated people says it was an error. January 23, 2025. https://www.lpm.org/news/2025-01-23/ky-lawmaker-introduces-bill-to-restrict-blood-donations-from-covid-vaccinated-donors
⁸ Sharma D, Booth GS, Jacobs JW, et al. Directed donations for unvaccinated blood: a departure from evidence-based medicine associated with clinical harm, resource waste, and oversight gaps in a two-year single-center series. Transfusion. 2026. https://doi.org/10.1111/trf.70195
⁹ Jacobs JW. How physicians like me are grappling with requests for unvaccinated donor blood. STAT News. June 11, 2025. https://www.statnews.com/2025/06/11/unvaccinated-blood-donations-covid-directed-donors-research-safety/