
You usually get this envelope in the mail about three weeks after you get home, sometimes four. Inside it is a document called an Explanation of Benefits, or EOB, which is one of those terms in healthcare that means almost the opposite of what it says. A little while later comes the itemized statement that could be mistaken for a novella. The numbers (codes you assume) are opaque, the descriptions abbreviated into near-meaninglessness, and if you have never seen one before, your first instinct is that you are reading it wrong. Each line has a billed amount, an allowed amount, and an amount you owe, three different numbers whose relationship to each other came out of a negotiation your hospital and your insurer conducted without you.
Most people look at the dollar sign on the bottom in the little box and try to ignore the icy dread creeping in.
The bill earns every bit of that. Reading it is like going over a contract written in a foreign language, where you know the words, but their meaning flies over your head. You try googling or ChatGPT’ing it, but that just makes matters worse. Whole industries—legitimate and otherwise—exist to help patients make sense of it all. One such is a man who goes by Hunter, or @hxxntrr, on X. A post of his collected 166,000 views about hospital billing that, naturally, ends with a link to his credit repair business. The views he garnered make sense given how thoroughly the healthcare system has earned its reputation for confusion, and that reputation did not come from nowhere. The system nurtured it carefully over decades.
the hospital you were born in charged your mother $40 for the first time she held you
— hunter (@hxxntrr) March 25, 2026
it's called "skin-to-skin contact" and there's a billing code for it. CPT 99460. your mother went through labor, pushed a human being out of her body, and the hospital charged her forty dollars…
Hospital bills draw from two coding systems that have different purposes. CPT codes, which stands for Current Procedural Terminology, describe what has been done to a patient. This can be many things, from an office visit to a physician's interpretation of your MRI. HCPCS codes (pronounced "hick-pix" in the trade) cover supplies, drugs, and equipment. The warming blanket in the recovery room has a HCPCS code. So does the bag of saline dripping into your arm. The two systems are maintained by different organizations and reimbursed under different rules, which matters a lot when you are trying to figure out what that line item is that’s staring up at you.
The problem is Hunter treats both systems as interchangeable, throwing them all into one CPT box. His unfamiliarity with coding references is where his argument slips drastically.
In his post, he writes that CPT 99460 is the billing code for "skin-to-skin contact," meaning this is the charge that lets hospitals bill a mother $40 for the first time she holds her newborn. The reality of this code is that it is used for the initial hospital or birthing center care, per day, for evaluation and management of a normal newborn infant.² Clinicians assign it to the first checkup of a baby, not for allowing the mother to hold her baby.
Where this particular piece of misinformation comes from is a reddit post from 2016. A Utah father named Ryan Grassley posted his hospital bill after his son was born via cesarean section. One line item read "skin to skin after c-sec: $39.35."¹ Utah Valley Hospital explained that the charge covered an additional nurse brought into the operating room so that Grassley's wife, lying splayed open on a surgical table, could safely hold the baby.¹ Charging it for the act of holding the baby is a different claim entirely, and a false one. Hunter attached the wrong code to a decade-old story and framed it as current fact.
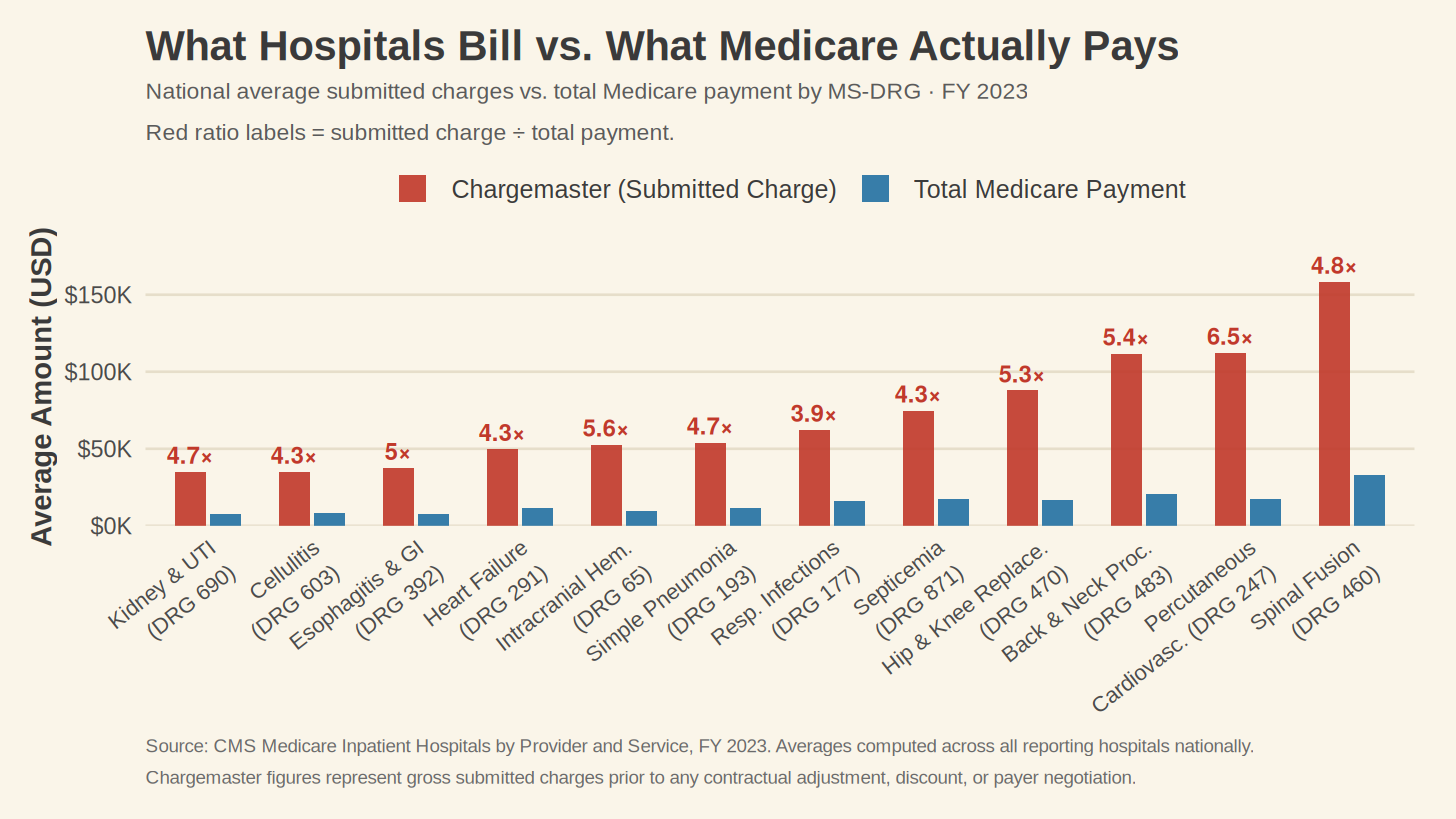
His chargemaster argument runs in the same direction. He posts side-by-side comparisons of wholesale supply costs against hospital billed charges, a saline bag that costs $0.86 to manufacture showing up on a bill at $400 to $900, and calls the difference fraud. Before laying out where that breaks down, the record needs to be clear on one point: chargemaster prices in this country are indefensible. Across twelve high-volume diagnosis-related groups in fiscal year 2023, the ratio of submitted charges to total Medicare payment ran from 3.9 to 6.5.⁵ For a percutaneous cardiovascular procedure, hospitals submitted an average charge of $112,338 and Medicare paid $17,170.⁵ For a spinal fusion, $158,444 submitted against $32,881 paid.⁵
What Hunter does not tell his readers is that the chargemaster price is not what most people pay. For patients with insurance, it functions less like a price and more like an opening bid in a negotiation that took place long before the service was rendered.
Hospitals bill for the nurse who verified the order against the patient's chart, threaded the line, set the drip rate, monitored the site, and documented all of it in the EHR. The pharmacy system that caught the interaction with the patient's blood thinner before the bag was hung charges for itself too. The $0.86 is the price of the sodium chloride. The $400 covers the clinical labor and the infrastructure that keeps the sodium chloride from killing anyone. Calling the difference between those two numbers fraud requires collapsing a supply cost and a service cost into one category and pretending they are the same thing.
Medicare pays hospitals based on diagnosis-related groups, or DRGs. When a Medicare patient is admitted, the clinical documentation gets coded, run through grouping software, and the hospital receives a set payment for that DRG regardless of what the chargemaster says. A hospital could double its chargemaster prices tomorrow, and its Medicare reimbursement would not change. The number on the hospital's website and the payment it receives operate in almost entirely separate systems.
Private commercial insurers negotiate contracted rates that land between the chargemaster price and the Medicare rate, closer to Medicare for smaller systems and substantially higher for large regional providers who can credibly threaten to walk away. That contracted rate becomes the allowed amount on your Explanation of Benefits. When you see a chargemaster charge of $900 and an allowed amount of $180 on the same line, the $720 difference was always going to disappear. The system required the $900 to exist so the $720 could be erased.
The patients most exposed to chargemaster prices are the ones without insurance, because they have no contracted rate standing between the bill and the balance. For them, the chargemaster is not a fiction, and Hunter’s anger at it is warranted. Every nonprofit hospital is required under Section 501(r) of the Internal Revenue Code to maintain a financial assistance policy and screen patients for eligibility before pursuing collections. He is right about that. The other parts, though, are buried under errors that sound credible, which makes the whole thing harder to trust.
Hunter assumes that if patients could see what hospitals charge, they could protect themselves. A federal rule that took effect in January 2021 tested that theory, requiring hospitals to post their prices publicly so patients could shop for care the way they shop for flights to grandma’s house. The analogy collapsed faster than a deck of cards. Airfares are the same seat sold at different prices. A hospital service is a different product for nearly every patient, priced by plan, provider, and contract terms that neither party is required to disclose to the patient. Insurers read the posted data extensively. Patients do not.
There is no evidence that patients use posted prices to make care decisions. Patients seeking imaging passed an average of six lower-priced facilities on the way to their appointment, following their physician's referral rather than any price search.³ A 2024 HHS Inspector General report found that 37 of 100 sampled hospitals were not meeting the posting requirements, with an estimated 46% of all required hospitals out of compliance nationwide.⁴ That is worth fixing. Whether fixing it would change what patients pay requires a different argument than the one the price transparency rule was built on.
Even a fully posted price cannot tell a patient what they will owe, because the number requires knowing their specific plan, where their deductible stands, whether the treating provider is in-network, and how the payer will handle the codes assigned. A patient reading a posted cost is in the same position as Hunter reading CPT 99460. The number is there, but the context that makes it meaningful is not.
Hunter latched onto patient confusion and monetized it. The confusing system, the inflated prices, the buried charity care policy were all available to him, and he chose the version that would get the most clicks rather than the version that would help a frightened patient understand their bill.
That itemized statement is probably still in your house, still in its envelope, because you have not been able to bring yourself to open it. A code you do not recognize is on it, attached to a charge that does not look rational. You cannot know whether it is wrong or whether you just do not understand what you are looking at, and that uncertainty is not a failure on your part. None of it was designed with you in mind.
Hunter knew that. He extended a hand to the person standing at the counter anyway, and was not careful about what he put in it.
References
- Ortega T. Utah father charged $39 to hold newborn after C-section birth goes viral. CBS News. October 6, 2016. https://www.cbsnews.com/news/utah-hospital-charges-mom-dad-39-to-hold-baby/
- American Medical Association. CPT code 99460: Initial hospital or birthing center care, per day, for evaluation and management of normal newborn infant. In: CPT Professional Edition. Chicago, IL: American Medical Association; 2024.
- Chernew M, Cooper Z, Larsen-Hallock E, Morton FS. Physician agency, consumerism, and the consumption of lower-limb MRI scans. J Health Econ. 2021;76:102427. doi:10.1016/j.jhealeco.2021.102427
- US Department of Health and Human Services Office of Inspector General. Not All Selected Hospitals Complied With the Hospital Price Transparency Rule. Washington, DC: HHS OIG; November 2024. https://oig.hhs.gov/reports/all/2024/not-all-selected-hospitals-complied-with-the-hospital-price-transparency-rule/
- Centers for Medicare and Medicaid Services. Medicare Inpatient Hospitals by Provider and Service, FY 2023. CMS.gov. https://data.cms.gov/provider-summary-by-type-of-service/medicare-inpatient-hospitals/medicare-inpatient-hospitals-by-provider-and-service