Robert F. Kennedy Jr.. Well, there he goes again.
The man who loves to submerge himself in a polar plunge tub—in 501s, no less—whilst downing a large glass of full-fat milk with his pal, Kid Rock, is not exactly someone who thinks too much about how things look. Case in point, on February 27th, during an appearance on the Joe Rogan Experience, he mentioned that he has ADHD.
On the show, he brought up this little factoid because Rogan was explaining why he wears headphones during interviews. As he says, they lock him in, filter out ambient noise, and help him stay focused on whomever is sitting across from him. Personally, I love this detail about him. Personally, I can’t relate for obvious reasons, but Kennedy’s response landed without hesitation.
“I have ADHD. I had 11 siblings and I have seven kids. So I can work, I can focus. No matter what.”
The diagnosis, in Kennedy’s telling, is practically a qualification for the job and the reason he can concentrate under any conditions rather it being something he manages around. Which is a fascinating thing for the head of HHS to say to tens of millions of listeners, particularly given that he has built a career on the claim that the public health establishment cannot be trusted with its information. He just contributed, in a small but nonzero way, to the single most culturally overloaded diagnosis in American life.
I don’t think he thought this through. Is it a big deal? Well…okay, kinda sorta. It depends.
The man may well have ADHD; that is not in dispute. The condition is absolutely real, and its presentation has a wider range than Fenway's Green Monster. High-functioning adults with ADHD hold hugely influential positions in every professional field. Whether his self-reporting is accurate is beside the point, because what matters is that in 2026, a cabinet secretary can drop a clinical diagnosis into a podcast conversation and move on before any competent interviewer has time to ask a single follow-up question, and nobody in the room finds that strange.
I can glance at my Substack feed and garner from the bios of the writers that ADHD has become something close to a professional identity marker. This, in part, is supposed to explain why people, at 2 a.m., fall down a rabbit hole that somehow becomes the best writing they’ve ever done in their life. I have no doubt that most of these writers are not wrong about their experiences in describing how their brains work. The question is whether ADHD is still the right word for what they are describing, or whether the label has gone so far kilter that it is now doing an entirely different job.
Oprah famously gave away cars. The internet has been considerably more generous with this diagnosis:
You have ADHD. YOU have ADHD! Everyone has ADHD!
But, honestly—and to no surprise—the data tells a far more complicated story.
The distance between who meets the right criteria and who have latched onto the label as their own is not a semantic twist. When that gap gets that wide, it corrupts the infrastructure public health depends on to understand what the hell is going on. What the data cannot show you is how much of that surge in adults [see below] was generated by a shadow diagnostic system that feeds directly into the clinical record without being subject to any of the quality controls. In other words, the numbers cannot tell the difference between a real diagnosis and a rubber stamp.
Direct-to-consumer telehealth platforms are absolutely amazing, and I love them and what they are doing; but they make money when they diagnose and prescribe, which means the encounter has a financial stake in its own outcome.
This is worth understanding because it is not as obvious as it looks.
Telehealth platforms built for volume use encounter templates structured around symptom checklists, which means the clinician is often working through a dropdown menu rather than conducting a clinical interview. The checklist produces documentation, which supports a code, which enters the record. Nobody in that chain did anything technically wrong, and the data has no way to know that the judgment was outsourced to a form. The NHIS (National Health Interview Survey) does not know if your diagnosis came from a three-hour neuropsychological evaluation (as it should have) or an intake form from an ad you saw on Facebook. The ICD-10 code looks identical regardless.
Sort of the Spearmint Gum twins, except one of them never went to medical school.
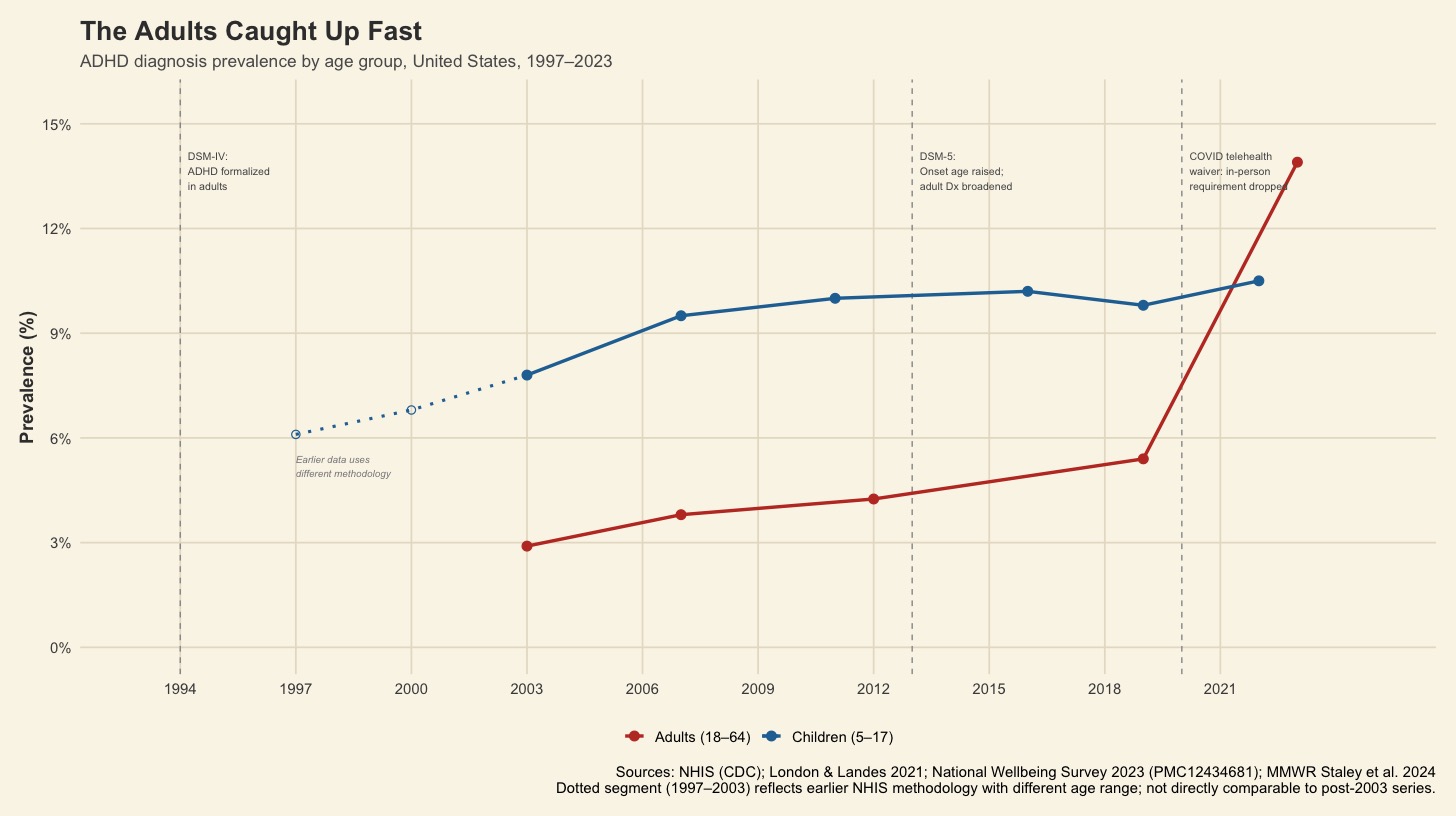
[Chart: The Adults Caught Up Fast — ADHD diagnosis prevalence by age group, United States, 1997–2023]
Our first instinct when seeing a prevalence curve shooting up the way this one does is not necessarily alarm, even tho my jaw hit the floor. The suspicion is much less than that than it is about what the numbers are measuring, because a real population-level increase in a neurodevelopmental condition would mean needing a biological explanation, which then means something environmental or genetic changed in enough of a way to move the curve so dramatically in that short of a window. No such explanation exists for ADHD.
What does exist are structural changes that made the diagnosis easier to get, alongside a shift in culture in how everyday people claim the ADHD label for themselves. Those two things have been feeding each other long enough that the data doesn’t know which way is Tuesday.
The DSM-IV formalized adult ADHD as a category in 1994, which sounds like ancient history (making me feel old) until you consider that an entire generation of adults grew up without that option available to them. When the DSM-5 came into this world with great gusto in 2013, it changed the required age of onset of symptoms from seven to twelve and knocked the adult symptom threshold down one from six criteria to five. Adults present with a different clinical picture than children, and women had been systematically underdiagnosed because the earlier hyperactivity-focused criteria were built around the behavioral presentation most commonly found in young boys.
The researchers who pushed for those changes had real reasons in a clinical sense, and the new and improved criteria reached populations that had been missed by the system for decades. What nobody anticipated was that the criteria would loosen up at the same time telehealth was removing the last barrier from getting diagnosed.
When the pandemic arrived in 2020, the DEA waived the in-person requirement for controlled substance prescribing, which means a patient who suspected they had ADHD could schedule a telehealth appointment, describe their symptoms to a doctor they’ve never met in a setting which has no way of observing behavior across multiple contexts, and get, as my husband calls it, “meth-by-mail” by the weekend. Many of those patients really, really do have ADHD. However, others just have anxiety, or burnout, or are just going through a thing while staring at screens for twelve hours a day. All of which can produce symptoms that look, from a brief telehealth intake, completely similar to inattentive ADHD. Detecting more cases is not the same thing as more cases out in the wild, and the public health surveillance infrastructure cannot tell the difference.
A diagnosis does not get into the public health record because someone mentions it on a podcast, or puts it in a Substack bio, or reports it when a survey interviewer asks whether a healthcare professional ever told them they had the condition. The NHIS question does the heavy lifting in the prevalence chart by asking whether a doctor or a professional-someone-else ever told you that you had ADHD. This is a very reasonable thing to ask on a population survey, but it cannot tell the difference between a diagnosis that took months of evaluation and one that came up in passing during a telehealth appointment. Both answers are yes, and both enter the prevalence estimate carrying identical weight statistically speaking.
For a diagnosis to be correctly coded, the clinician has to document it with enough specificity to support an ICD-10 code:
- F90.0 for predominantly inattentive presentation,
- F90.1 for predominantly hyperactive-impulsive,
- F90.2 for combined.
The criteria for those codes need symptom onset before age twelve, functional impairment in at least two settings, and symptoms not better explained by another condition (ironically, like hearing impairment—hello, Andrew). When those standards are met and documented, the code is considered viable; but when a patient arrives at an encounter already convinced they have ADHD and the clinician documents the history without an evaluation, that code enters the record anyway, and is indistinguishable in the aggregate data.
The diagnostic problems are pulling each other in opposite directions like in a tug-o’-war, which is why the picture doesn’t have a clean narrative that we can act on. A working-age adult with reasonable good insurance, therefore access to a telehealth, is going through a completely different experience than an uninsured adult in a rural county with a three-month wait for their PCP and no one in the system with expertise in adult neurodevelopmental conditions. The 13.9% prevalence figure from the 2023 National Wellbeing Survey is real in the sense that not quite a seventh of working-age adults surveyed reported ever receiving the diagnosis, but what it cannot tell you is how many of those diagnoses are from a clean evaluation versus a fifteen-minute intake, or how many people in underserved communities have the condition without documentation because the infrastructure to identify them was never funded.
What is happening in the writing community is worth looking at. The ADHD symptom profile maps—all too well—onto the romantic mythology of the creative mind, where obsessive focus is a sign of genius and distractibility is just curiosity and the inability to stop researching a topic at 2 a.m. is just passion rather than dysregulation. For writers especially—and, in many ways, I can relate as a fiction writer—an ADHD label gives them a vocabulary for understanding how they are pieced together. Adopting it feels less like a verdict than like finally finding the right word in a phrase you just couldn’t figure out. It essentially becomes a credential that explains not just how the brain is constantly misfiring but how it produces their work, which is very different from something the DSM was designed to do. We’ve been blurring these together so long that it’s not so straightforward anymore because the downstream cost is in datasets very few will ever see.
I think Kennedy’s position makes this so real in a way that Substack bios can’t. He’s spent years insisting Big Medicine cannot be trusted to interpret its own evidence, and his relationship with any sort of health data has been, to put it mildly, selective. He now oversees the agencies responsible for maintaining the surveillance systems that generate that data, setting expectations for what gets measured, what is funded, and what gets allowed to degrade (38 datasets are missing from the CDC, but I digress). His ADHD claim will not move so much as a single ICD-10 code, but the cultural environment it feeds, one in which self-identification distorts diagnostic criteria, makes it harder to fix when the person making an offhand comment also controls the budget of those doing the measuring.
Adults who receive real diagnoses in the past decade were right to seek them, and the condition itself is not in question here. The people who were told they were scattered or just being difficult or simply not trying hard enough, are finally receiving a diagnosis in their thirties, or even sixties, and finding it genuinely relieving, are not casualties of cultural drift. They are casualties of criteria that had been built around the wrong population, and the DSM-5 revisions that reached them were overdue.
What went wrong is that the expansion happened without the infrastructure to track what it was measuring, and the cultural adoption of the label shot so far ahead of the clinical system that the two are now only vaguely tied.
When Kennedy dropped his diagnosis, he was doing something millions of people do every day which is using a clinical label as shorthand for something about how their mind works to a community where that shorthand is embraced. He runs HHS, though. That much influence, wielded by someone who has already demonstrated a willingness to use medical information selectively, gives his disclosure a weight that a Substack bio simply cannot compete with.
The Oprah joke works. The difference is that when Oprah gave something away, she knew she was doing it.
Sources: Joe Rogan Experience #2461, February 27, 2026. NHIS (CDC). London & Landes 2021. National Wellbeing Survey 2023 (PMC12434681). MMWR Staley et al. 2024. DSM-IV (1994); DSM-5 (2013). NCHS Data Brief No. 499, March 2024.
The R code and data used to produce this chart are available on GitHub.